


Abstract
We compared monotherapies and combinations of therapies that regulate G-protein–coupled receptors (GPCRs) with respect to their abilities to inhibit early stages of diabetic retinopathy (DR) in streptozotocin-diabetic mice. Metoprolol (MTP; 0.04–1.0 mg/kg b.wt./day), bromocriptine (BRM; 0.01–0.1 mg/kg b.wt./day), doxazosin (DOX; 0.01–1.0 mg/kg b.wt./day), or tamsulosin (TAM; 0.05–0.25 mg/kg b.wt./day) were injected individually daily for 2 months in dose-response studies to assess their effects on the diabetes-induced increases in retinal superoxide and leukocyte-mediated cytotoxicity against vascular endothelial cells, both of which abnormalities have been implicated in the development of DR. Each of the individual drugs inhibited the diabetes-induced increase in retinal superoxide at the higher concentrations tested, but the inhibition was lost at lower doses. To determine whether combination therapies had superior effects over individual drugs, we intentionally selected for each drug a low dose that had little or no effect on the diabetes-induced retinal superoxide for use separately or in combinations in 8-month studies of retinal function, vascular permeability, and capillary degeneration in diabetes. At the low doses used, combinations of the drugs generally were more effective than individual drugs, but the low-dose MTP alone totally inhibited diabetes-induced reduction in a vision task, BRM or DOX alone totally inhibited the vascular permeability defect, and DOX alone totally inhibited diabetes-induced degeneration of retinal capillaries. Although low-dose MTP, BRM, DOX, or TAM individually had beneficial effects on some endpoints, combination of the therapies better inhibited the spectrum of DR lesions evaluated.
SIGNIFICANCE STATEMENT The pathogenesis of early stages of diabetic retinopathy remains incompletely understood, but multiple different cell types are believed to be involved in the pathogenic process. We have compared the effects of monotherapies to those of combinations of drugs that regulate GPCR signaling pathways with respect to their relative abilities to inhibit the development of early diabetic retinopathy.
Introduction
Despite many years of research, the pathogenesis of early stages of diabetic retinopathy (DR) remains incompletely understood. Numerous postulates have been put forth to explain the early development of the retinopathy based on single molecular abnormalities (Kowluru and Mishra, 2015; Tonade et al., 2017; Liu et al., 2019a; Sahajpal et al., 2019) or abnormalities in single retinal cell types, including endothelial cells (ECs), pericytes, ganglion cells, Müller cells, retinal pigment epithelium, and retinal photoreceptor cells (Kern and Barber, 2008; Simo et al., 2010; Xu et al., 2011; Beltramo and Porta, 2013; Wang et al., 2015; Tonade et al., 2017; Simo et al., 2018; Liu et al., 2019a; Kowluru and Mohammad, 2020). Therapeutic approaches to inhibit the retinopathy have focused primarily on targeted treatment of only single defects. Since redundancy of biologic pathways allows cells and tissues to compensate when several aspects of that system are perturbed (Berger and Iyengar, 2009), however, therapy with a single drug is less likely to normalize a perturbed system than is a combination of drugs that act on different targets within the same or even unrelated networks.
G-protein–coupled receptors (GPCRs) comprise a large diverse superfamily of membrane proteins encoded by more than 800 genes (Fredriksson et al., 2003) that transduce a wide variety of extracellular signals, including photons, ions, small organic molecules, and proteins, into intracellular second messengers through activation of one or more G-proteins, including the Gs, Gi, and Gq subtypes (Marinissen and Gutkind, 2001). Often, agonism at Gs-coupled GPCRs increases the activity of adenylyl cyclase, leading to increased generation of cAMP, whereas agonism at Gi-coupled receptors has an opposite (inhibitory) effect. The Gq-coupled receptor-signaling pathway differs from Gs- and Gi-coupled receptors in that it signals via the phospholipase C pathway, eventually leading to Ca2+ release from the endoplasmic reticulum and activation of NADPH oxidase (Yamamori et al., 2000; Brown, 2007; Inoue et al., 2008).
In diabetes, a number of GPCR-regulating drugs [including doxazosin (DOX), prazosin, guanabenz, lofexidine, and RO 04-6790] that regulate diverse signaling pathways downstream of the different G-proteins all had the common effect of inhibiting the diabetes- or glucose-induced increase in superoxide in retinal cells (Du et al., 2015). This is important because oxidative stress has been implicated in the pathogenesis of DR (Kowluru et al., 2001; Kanwar et al., 2007; Berkowitz et al., 2009). Moreover, daily administration of DOX [an α1-adrenergic (Gq)-receptor antagonist (Hamilton et al., 1985)] for 8 months statistically significantly inhibited molecular abnormalities and the capillary degeneration that is characteristic of DR (Du et al., 2015).
Study of transcript abundance has shown that a subset of GPCRs is highly expressed in retina (Chen et al., 2016b) and that targeting those abundant receptors with agonists or antagonists resulted in protection from retinal degeneration secondary to bright light or Stargardt disease (Chen et al., 2013, 2016b; Orban et al., 2017; Leinonen et al., 2019). Moreover, simultaneous administration of a Gi-receptor agonist, bromocriptine (BRM), along with the Gs- and Gq-receptor antagonists metoprolol (MTP) and tamsulosin (TAM), respectively, was found to exert a better-than-additive (synergistic) protection of photoreceptor cells in those disease models (Chen et al., 2013, 2016b; Orban et al., 2017; Leinonen et al., 2019).
In the present report, we evaluated the effects of MET, BRM, TAM, or DOX monotherapies on molecular abnormalities that are believed to contribute to the development of DR and then investigated whether combinations of these drugs inhibited the development of long-term pathology of DR (such as retinal permeability, capillary degeneration, and visual dysfunction) better than did the monotherapies. These drugs were selected not based on any known biochemical or functional abnormalities downstream of those receptors in diabetes but instead based on the abundance of their receptors in the retina and the previously reported beneficial effects of these drugs in retinal degenerative diseases.
Materials and Methods
Animals and Diabetes
All experiments followed the guidelines set forth by the Association for Research in Vision and Ophthalmology Resolution on Treatment of Animals in Research and by the institutional Animal Care and Use Committee. Insulin-deficient diabetes was induced in randomly selected 2-month-old fasted male C57BI/6J mice (Jax 000664, Bar Harbor, MA) by intraperitoneal injections of streptozotocin (60 mg/kg b.wt.) on 5 consecutive days. Insulin was given as needed (0–0.2 units every 2–3 days) to maintain body weight while allowing chronic hyperglycemia, polyuria, and hyperphagia. Female rodents are resistant to the diabetogenic effects of streptozotocin (Rossini et al., 1978; Leiter, 1982), so only males were used in the present study. Blood glucose and HbA1c were measured as reported previously (Lee et al., 2013; Tang et al., 2013b). Diabetic mice and age-matched nondiabetic control mice were studied after 2 months of diabetes or 8 months of diabetes (i.e., 4 and 10 months of age).
Two experiments were conducted. The first involved daily treatment of diabetic mice for 2 months (a duration of diabetes that results in molecular and some functional changes in the retina, but retinal vascular abnormalities, such as increased permeability and degeneration, have not yet developed); the second study involved drug treatment daily for 8 months of diabetes (a duration of diabetes that results in a statistically significant increases in retinal vascular permeability and degeneration compared with nondiabetic controls) (Feit-Leichman et al., 2005).
Drug Studies
Dose-response curves were generated by injecting different doses of MET (0.04–1.0 mg/kg b.wt./day), BRM (0.01–0.1 mg/kg b.wt./day), DOX (0.01–1.0 mg/kg b.wt./day), and TAM (0.05–0.25 mg/kg b.wt./day) into diabetic mice daily intraperitoneally for 2 months. These drugs were selected for their ability to modulate signaling systems downstream of GPCRs expressed in high abundance in the retina (Chen et al., 2013) and for previously reported beneficial effects on the retina in diabetes and retinal degeneration (Chen et al., 2013, 2016b; Du et al., 2015; Orban et al., 2017; Leinonen et al., 2019). These 2-month dose-response studies were conducted to evaluate the effects of the individual drugs on diabetes-induced retinal oxidative stress and other molecular abnormalities that have been implicated in development of the retinopathy. From these studies, we identified also a low dose of each drug that individually had little or no effect on the retinal oxidative stress [labeled dose of minimal inhibition of retinal oxidative stress (DMIox)] and used that dose of each drug in 8-month studies to determine whether combinations of the drugs more effectively inhibited the early stages of DR than did monotherapies. We conducted the long-term study using 11 experimental groups as summarized in Table 1. All therapeutics were administered at identified doses daily by intraperitoneal injection in DMSO. An initial 2-month study with diabetic mice treated with and without DMSO showed no statistically significant difference on retinal superoxide, so diabetic control animals were untreated in subsequent studies. Drugs were obtained from Sigma-Aldrich (St. Louis, MO).
Clinical data of experimental groups over 8 months of diabetes
Retinal Superoxide
Freshly isolated retinas were incubated in 200 µl of Krebs-Hepes buffer, pH 7.2, with 5 mM or 25 mM glucose for 5 minutes at 37°C in 5% CO2. Luminescence indicating the presence of superoxide was measured 5 minutes after addition of lucigenin to 0.54 mM (Du et al., 2003; Kern et al., 2007; Gubitosi-Klug et al., 2008; Du et al., 2010; Kern et al., 2010; Veenstra et al., 2015). Luminescence intensity is reported in arbitrary units per milligram protein.
Immunoblots
Retinal homogenates were separated by SDS-PAGE and incubated with either anti–intercellular adhesion molecule-1 (ICAM1; 1:2000 dilution; MAB796; R&D Systems, Minneapolis, MN) or the anti–inducible isoform of nitric oxide synthase (iNOS; 1:1000 dilution; SC-7271; Santa Cruz Biotechnology, Inc., Santa Cruz, CA). Protein levels were quantified relative to β-actin loading controls (1:3000 dilution; AB8226; Abcam, Inc., Cambridge, MA) in the same samples.
Optokinetic Assessment of Visual Function
The maximum spatial frequency that resulted in head tracking was determined as the spatial frequency threshold. After 2 months of diabetes, contrast sensitivity was measured at a single spatial frequency (0.064 cycles/degree) with the Virtual Optomotor system, as previously described (Prusky et al., 2004; Lee et al., 2013; Liu et al., 2015b). The grader was masked with respect to the animals’ experimental group. Although nondiabetic mice could be differentiated from diabetic animals based on body weight, investigators could not discern drug treatment group identity (Li et al., 2012; Talahalli et al., 2013; Tang et al., 2013a, 2013b; Tian et al., 2013; Veenstra et al., 2013).
Leukocyte-Mediated Cytotoxicity of ECs
Immortalized retinal ECs (Su et al., 2003) were grown in control medium (Dulbecco’s modified Eagle’s medium with 5 mM glucose) containing 10% serum. The serum concentration was reduced to 2% just before cells were placed either in normal glucose (5 mM) or high glucose (30 mM). Media was changed every other day for 3 days. When cells reached 80% confluence (∼300,000 cells), freshly isolated leukocytes from blood (100,000 cells) were added and incubated for additional 6 hours, after which cells were collected and washed with PBS. Cells were stained with an antibody against CD144 (1:50 dilution, BD Biosciences Pharmingen, San Diego, CA) to identify ECs, and the viability of the ECs was identified by flow cytometry based on 7-aminoactinomycin D (BD, San Diego, CA) staining. EC death was expressed as the percentage of ECs that stained positively with dye. Approximately 10,000 cells were counted in each sample. Experiments were repeated twice with similar results each time.
Capillary Degeneration
Diabetes-induced vascular pathology was measured in retinas from diabetic animals for 8 months and their age-matched controls, as described previously (Li et al., 2011; Li et al., 2012; Veenstra et al., 2013). Briefly, formalin-fixed retinas were digested with 40 U/ml elastase (Calbiochem, San Diego, CA) (Veenstra et al., 2015). When totally freed of neural cells, the isolated retinal vasculature was laid out on a glass microscope slide, dried, and stained with hematoxylin and periodic acid-Schiff. Degenerated (acellular) capillaries were quantified in a masked manner in 6–7 field areas corresponding to the midretina.
Permeability
Retinal permeability was measured in the other eye from animals in the long-term studies using a fluorescently labeled tracer as described previously (Antonetti et al., 1998; Du et al., 2015; Liu et al., 2015a; Liu et al., 2019b). Briefly, sterile fluorescein isothiocyanate (FITC)– bovine serum albumin (BSA; 50 µg/µl; Sigma-Aldrich A9771) in phosphate-buffered saline (NaCl, 0.138 M; KCl, 0.0027 M; pH 7.4) was injected into the tail vein of mice at 100 µg/g b.wt. The dye circulated for 20 minutes before blood samples were collected and eyes were enucleated. One eye was fixed in ice-cold 4% paraformaldehyde, infused with sucrose, and then frozen in Optimal Cutting Temperature compound. in isopentane on dry ice. Retinal cryosections were imaged by fluorescence microscopy. Two sections per eye were imaged equidistant on either side of the optic disc in the inner and outer plexiform layers to generate an average image pixel density in the neural retina exclusive of any vessels from a total of four images. Relative average fluorescence values were normalized to the relative plasma fluorescence for final determinations of retinal dye accumulation.
Statistical Analyses
Data are expressed as mean ± S.D. All statistical analyses were performed by ANOVA, which was followed by Fischer's least significant difference (LSD) post hoc test (StatView, SAS Institute, Inc.). Intergroup comparisons in the ANOVA post hoc tests were made between all groups with appropriate correction for multiple comparisons, but results are reported here only for the comparisons of Diabetic control versus Nondiabetic control and Diabetic control versus drug-treated Diabetic except as noted in the text. Values of P < 0.05 (two-tailed) are considered statistically significant. Individuals performing assays were masked as to which group the animals were in, with the exception that nondiabetic animals could be differentiated from patients with diabetes based on body weight during visual function tests (but it was impossible to visibly differentiate among the various diabetic groups). The 2-month studies served both a hypothesis-testing role (GPCR-modifying drugs inhibit diabetes-induced increase in retinal superoxide) stated prior to the onset of the study and an exploratory role (determine the DMIox for each drug). The 8-month study was hypothesis-testing (combinations of therapies that modify GPCR signaling better inhibit DR than do monotherapies). All comparisons tested a prespecified statistical null hypothesis that there was no statistically significant difference between the diabetic control group and patients with diabetes treated with GPCR-modifying drugs. Use of the term “significant” in this manuscript always refers to statistical significance. Group sizes needed at the end of the experiment (n = 6 per group) were estimated by sample-size analysis based on previously reported differences between diabetic and nondiabetic controls with respect to retinal capillary degeneration, and initial group sizes were then increased in anticipation of some mortality or reversal of diabetes. The analysis steps had been decided before seeing the data. Sample sizes were unequal at the time of sample collection because of tissue availability or mortality.
Results
Diabetes
As intended, all diabetic groups had HbA1c and blood glucose concentrations that were greater than those found in age-matched, nondiabetic controls. None of the drug treatments had an effect on glycemia. Average body weights, nonfasting glucose levels, and HbA1c concentrations for the animal groups in the 8-month experiment are summarized in Table 1. Mortality during the 8-month experiment also is summarized in the table. Clinical data from a representative 2-month study are shown in Supplemental Table S1 and were similar to those in the 8-month study.
Two-Month Diabetes
Diabetes of 2-month duration significantly increased retinal superoxide (P < 0.001; Fig. 1A). When MTP, BRM, DOX, or TAM were administered individually to diabetic animals for 2 months, the higher dosages tested of each drug significantly (P < 0.01) inhibited the diabetes-induced increase in retinal superoxide (Fig. 1B), providing evidence that pharmacologically targeting GPCRs protects the retina against oxidative stress in diabetes. To minimize the likelihood of undesirable side effects of these drugs and to determine whether combinations of the drugs resulted in additive or greater-than-additive inhibition of lesions of the retinopathy, we sought to identify a lower dose of each monotherapy at which there was little or no inhibition of the diabetes-induced increase in retinal superoxide. Based on the reported equation to convert the dose of each drug used in humans to a comparable dose for mice (Food and Drug Administration, 2005), the dosages used in the present study are below clinically used daily dosages, with the exception of TAM (see Supplemental Table S2). Using the data in Fig. 1B, an estimated ED50 for inhibition of the diabetes-induced increase in retinal superoxide was calculated for each of the individual drugs and is summarized in Table 2.

Individually administered drugs that modulate GPCR pathways inhibited the diabetes-induced increase in retinal oxidative stress. (A) Diabetes (Diab) of 2-month duration caused a 2-fold increase in the superoxide level in the retina compared with that in age-matched nondiabetic (N) controls. (B) Daily administration of MTP, BRM, DOX, or TAM individually to diabetic animals for 2 months totally inhibited the diabetes-induced increase in retinal superoxide at the highest concentrations administered. The lowest doses tested (also administered daily for 2 months) were less effective and led to the identification of a dose of each drug that was regarded as the DMIox reported in Table 2. The magnitude of the diabetes-induced increase in retinal superoxide shown in (A) applies also to all graphs in (B). In the panels, each hollow circle corresponds to data from an individual mouse, and the vertical bars depict group means. Sample size is indicated below each column. *P < 0.05; **P < 0.001 compared with diabetic control.
Drug dosages administered daily in 8-month study and estimated ED50
Whereas administration of any of the individual drugs for 2 months at their DMIox led to little or no inhibition of the diabetes-induced retinal oxidative stress, coadministration of MTP, BRM, DOX, or TAM with any other of the drugs (also at their DMIox) statistically significantly inhibited the retinal oxidative stress (Fig. 2). These data demonstrate what appears to be a greater-than-additive effect of the drugs against retinal oxidative stress in diabetes and provide evidence that signaling pathways regulated by adrenergic and serotonin and dopamine receptors contribute to diabetes-induced oxidative stress. Strikingly, however, the benefit of therapy combinations was less evident when BRM was substituted with a selective D2-like receptor agonist, pramipexole (Fig. 3).

Superadditive inhibition of retinal superoxide by combination therapies. By definition, daily administration of drugs individually at their DMIox for 2 months had little or no effect on the diabetes-induced retinal oxidative stress. Combinations with other test drugs (also at their DMIox), however, caused a marked (essentially total) inhibition of the oxidative stress. Nondiabetic (N) control = 100%. Sample size is indicated below each column. *P < 0.05; **P < 0.001 compared with diabetic control.

Replacement of BRM by a different dopaminergic Gi agonist [Pramipexole (Pram); selective to D2-, D3-, D4-receptors] resulted in less inhibition of retinal superoxide, even when combined with MTP and DOX. Pram was administered daily at two subefficacious doses (0.1 and 0.01 mg/kg/day) as a monotherapy and in combination with MTP and DOX (which were administered at their DMIox) for 2 months. As a monotherapy, Pram at the higher dose only modestly, albeit statistically significantly, inhibited the superoxide increase. Sample size is indicated below each column. *P < 0.05; **P < 0.001 compared with diabetic control. N, nondiabetic.
Diabetes of 2-month duration also significantly increased the expression of proinflammatory proteins iNOS and ICAM1 (both P < 0.05; Fig. 4; Supplemental Fig. S1). Both of these proinflammatory proteins have been implicated in the pathogenesis of vascular lesions in early DR (Joussen et al., 2004; Zheng et al., 2007). Individual drugs administered daily for 2 months at their DMIox did not inhibit diabetes-induced increases in iNOS or ICAM1, but many of the drug combinations did so, despite being at their DMIox (Fig. 4). In response to the drug combinations, the diabetes-induced increase in retinal iNOS was inhibited almost totally, and the increase in ICAM1 was inhibited by about half.
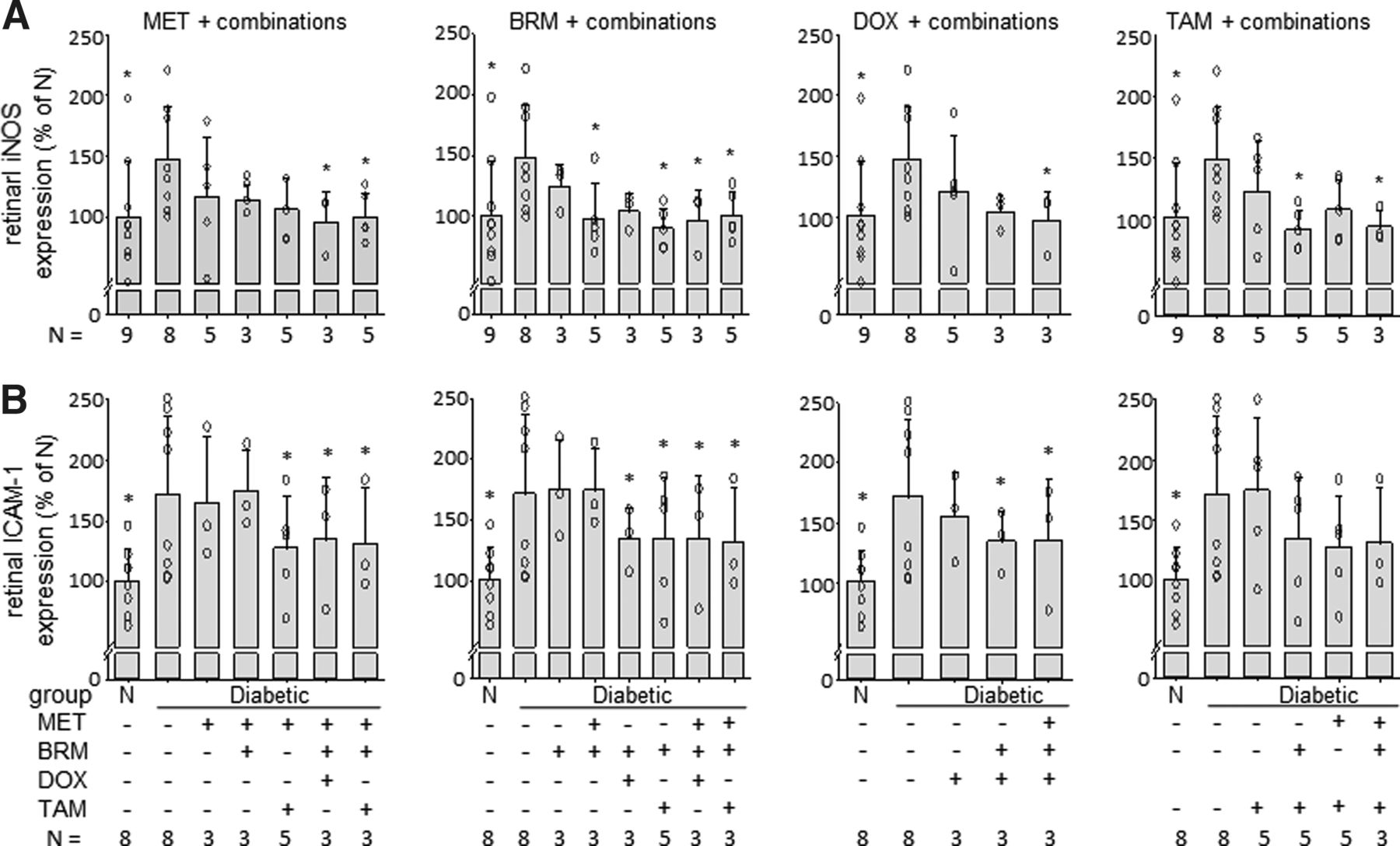
Effect of drugs on the diabetes-induced increase in expression of proinflammatory proteins in retina in diabetes. The diabetes-induced increases in expression of iNOS (A) and ICAM1 (B) in the retina were only partially inhibited by daily administration of MTP, BRM, DOX, or TAM individually at their DMIox, but these proteins in the retina were strongly inhibited by most combinations of the drugs. Representative Western blots are included in the Supplemental Fig. S1. Sample size is indicated below each column. *P < 0.05 compared with diabetic control. N, nondiabetic.
We previously implicated leukocytes as contributing to the development of vascular lesions in DR (Li et al., 2012; Talahalli et al., 2013; Tian et al., 2013; Veenstra et al., 2013), and the killing of retinal ECs by leukocytes from either patients who are diabetic (Tian et al., 2013) or diabetic mice (Li et al., 2012) has been demonstrated ex vivo. Because systemically delivered drugs do not affect only retinal cells, we assessed the effects of MTP, BRM, DOX, and TAM individually and in combinations on the leukocyte-mediated cytotoxicity against retinal ECs using leukocytes isolated from the blood of animals treated with drugs for 2 months. Daily administration of either MTP or BRM as monotherapies at their DMIox to diabetic animals did not statistically significantly inhibit leukocyte-mediated cytotoxicity against retinal ECs, but their combinations with other drugs did (Fig. 5). In contrast, DOX statistically significantly inhibited the diabetes-induced leukocyte-mediated EC death as a monotherapy and in any of the combinations tested (Fig. 5).

Leukocytes isolated from mice diabetic for 2 months caused more cytotoxicity to retinal ECs than did leukocytes from age-matched nondiabetic (N) mice. This effect was only partially inhibited (not statistically significantly) by MTP or BRM individually at their DMIox doses, but the inhibition was essentially total by DOX monotherapy or by the drug combinations. Leukocytes were collected from bone marrow of animals in the different experimental groups and were cocultured ex vivo with retinal ECs for 6 hours. EC death was quantified by flow cytometry. Sample size is indicated below each column. *P < 0.05; **P < 0.001 compared with diabetic control.
Contrast sensitivity and spatial frequency threshold are psychophysical measures that assess the function of retina-to-midbrain (superior colliculus) visual pathways. Diabetes for a 2–3-month duration in wild-type C57Bl/6J mice (4–5 months age) caused a significant decrease in both parameters of visual function compared with nondiabetic controls (Fig. 6; both P < 0.05). Daily administration of MTP alone or BRM + DOX or MTP + BRM + DOX all statistically significantly inhibited the diabetes-induced decrease in spatial frequency threshold. None of the therapies or combinations improved the diabetes-induced reduction in contrast sensitivity measurement at the single spatial frequency evaluated.

Impairment of visual function in diabetic C57Bl/6J mice compared with nondiabetic C57Bl/6J mice at 4–5 months of age (2–3 months of diabetes in appropriate animals) and effects of drugs at their DMIox. Spatial frequency threshold (A) and contrast sensitivity (B) were reduced slightly (but statistically significantly) in diabetic C57Bl/6J mice compared with nondiabetic (N) controls. Contrast sensitivity was measured only at a single fixed spatial frequency (at 0.064 cycles/degree). Daily administration of MTP monotherapy or BRM + DOX or MTP + BRM + DOX almost totally preserved spatial frequency threshold, but none of the monotherapies or combinations had a similar beneficial effect on the contrast sensitivity measurement. Sample size is indicated below each column. *P < 0.05 compared with diabetic control.
Eight-Month Diabetes
Based on the drug studies at 2 months of diabetes (described above), we initiated long-term studies using MTP, BRM, DOX, and TAM at their DMIox drug dosages. The drugs were administered individually or in combinations daily for 8 months to determine the effects of the drugs on clinically meaningful endpoints of DR.
As expected, diabetes of 8-month duration caused a statistically significant increase in the number of degenerated retinal capillaries (Fig. 7). Neither MTP nor BRM at their DMIox inhibited degeneration of retinal capillaries in diabetic mice over the 8-month period, but the capillary degeneration was statistically significantly inhibited by either DOX or TAM monotherapies at their DMIox. The triple combination therapies of either MTP + BRM + DOX or MTP + BRM + TAM also statistically significantly inhibited the diabetes-induced degeneration of retinal capillaries.

Diabetes-induced degeneration of retinal capillaries at 8 months of study. MTP, BRM, DOX, and TAM were administered daily at their DMIox doses individually or in combinations. (A) Graphical summary of the number of degenerated capillaries in midretina of nondiabetic and diabetic mice at 8 months of diabetes (10 months of age; sample size is indicated below each column). Individually at their DMIox doses, neither MTP nor BRM appreciably inhibited the capillary degeneration, but DOX or TAM monotherapies did statistically significantly inhibit the vaso-obliteration. Most combinations inhibited the capillary degeneration. (B–E) show representative photomicrographs demonstrating the retinal vasculature at the same age. (B) WT nondiabetic, (C) WT diabetic control, (D) DOX as a monotherapy, (E) MTP + BRM + DOX as a combination therapy. Degenerated retinal capillaries (acellular capillaries; illustrated by white arrows) are about 50% more numerous in WT diabetic mice than in WT nondiabetic mice. The effect of each of the other drugs or drug combinations to inhibit the capillary degeneration is assessed compared with the WT diabetic group. Calibration bar indicates 50 µm actual dimensions. *P < 0.05; **P < 0.001 compared with diabetic control. Mean ± S.D. N, nondiabetic; WT, wild type.
Diabetes of 8-month duration also significantly increased leakage of FITC-BSA into regions of the neural retina occupied by the vascular beds [inner plexiform layer (IPL) and outer plexiform layer (OPL)] (both P < 0.001; Fig. 8), and this permeability defect responded somewhat differently to therapies than did the capillary degeneration. Neither MTP nor TAM had any effect on leakage of FITC-albumin into the IPL or OPL, whereas BRM and DOX monotherapies at their DMIox very significantly inhibited the leakage defects (both P < 0.001). Because of the strong therapeutic effect of BRM and DOX monotherapies in this assay, none of the drug combinations showed a better inhibition of the permeability defect than those monotherapies. Nonetheless, the permeability defects were almost totally inhibited in diabetic mice treated with MET + BRM + DOX, and permeability in those animals was indistinguishable from Nondiabetic controls. BRM monotherapy was significantly more effective at inhibiting the permeability defect in both retinal layers than MET + BRM + TAM (P < 0.0002). Comparing the two triple therapies, MET + BRM + DOX was significantly more effective at inhibiting the permeability defect than was MET + BRM + TAM (P < 0.01 in both retinal layers). In contrast to the beneficial effect of DOX on permeability, TAM (the other Gq-linked inhibitor tested) had no such beneficial effect on retinal permeability in vivo unless combined with others of the tested drugs (Fig. 8).

Leakage of albumin into the neural retina in diabetes. Diabetes-induced degeneration of retinal capillaries at 8 months of study. Diabetes of 8-month duration more than doubled the accumulation of FITC-BSA in the (A) IPL and (B) OPL of the retina, as evidenced by diffuse green color in IPL and OPL. Bright green spots indicate FITC-BSA within retinal capillaries and are not included in the quantification for permeability determination. All drugs were administered daily at their DMIox. Neither MTP nor TAM inhibited the diabetes-induced defect in permeability, but both BRM and DOX totally and significantly inhibited the defect in both layers. (C–E) show representative photomicrographs illustrating fluorescence in the neural retina. (C) WT nondiabetic, (D) WT diabetic control, (E) MTP + BRM + DOX as a combination therapy administered daily to diabetic mice. FITC-albumin was injected intravenously, allowed to circulate for 20 minutes, and then fluorescence in areas of the IPL or OPL was quantified from retinal cross-sections. Calibration bar indicates actual dimensions. Sample size is indicated below each column. INL, inner nuclear layer; IPL, inner plexiform layer; ONL, outer nuclear layer; OPL, outer plexiform layer; RGC, retinal ganglion cell layer; ROS, rod outer segments. *P < 0.05; **P < 0.001 compared with diabetic control. Mean ± S.D. N, nondiabetic; WT, wild type.
Discussion
In the present study, we sought to investigate whether the use of multiple drugs that act on complimentary GPCR signaling systems might result in better inhibition of DR than can be achieved using a single drug therapy. When used alone, MET, BRM, DOX, or TAM significantly inhibited several diabetes-induced molecular abnormalities in the retina at the high doses tested and were less effective at lower doses.
Using a kinetic assay to study the effect of these drugs on G-protein activation by GPCRs, Chen et al. (2016b) reported that BRM activates dopamine receptors D4R and D2R as well as inhibiting the α1A-adrenergic receptor (ADRA1A). DOX was found to be a full antagonist for ADRA1A. TAM demonstrated complex activity on the four receptors, and MTP showed no agonistic or antagonistic effects on any of the four GPCRs tested. Knowledge about which receptors are being influenced by the drugs used and the biologic effects of those drugs is expected to provide insight into the molecular mechanism(s) by which pathology of DR develops and might be inhibited. The most likely explanation for the powerful effect of BRM is as a dopamine R2 agonist. Dopamine is known to counter Vascular Endothelial Growth Factor–induced permeability (Bhattacharya et al., 2008). The beneficial actions of DOX on diabetes-induced degeneration of retinal capillaries were reproduced also by pharmacologic inhibition of NADPH oxidase (Du et al., 2015), thus suggesting that superoxide generation or calcium release after hyperglycemia-mediated activation of ADRA1A is involved in the capillary degeneration.
Since oxidative stress has been implicated in the pathogenesis of at least the vascular lesions of DR, it was surprising that monotherapies of DOX or BRM at doses that did not inhibit retinal superoxide (DMIox) nevertheless caused a significant inhibition of retinal vascular permeability in diabetes. Likewise, degeneration of retinal capillaries was strongly inhibited by DOX monotherapy at a dose that did not inhibit retinal superoxide. Thus, the effect of a drug on retinal oxidative stress does not necessarily predict its effect on vascular or neural lesions of the retinopathy.
Individual drugs inhibited some lesions of the retinopathy but did not correct all of the retinal abnormalities in diabetes. BRM inhibited the retinal permeability defect in diabetes at the low dose tested but did not significantly inhibit the retinal capillary degeneration or visual dysfunction. MTP alone inhibited the loss of visual acuity as estimated from spatial frequency threshold but had no significant effect on either retinal capillary permeability or degeneration in diabetes. DOX inhibited the defects in capillary permeability and degeneration but showed no similar beneficial effect on visual function.
Previous studies showed that simultaneous administration of low doses of MTP, TAM, and BRM resulted in a synergistic (superadditive) inhibition of retinal photoreceptor cell degeneration (Chen et al., 2013, 2016b; Orban et al., 2017; Leinonen et al., 2019). Data in the present study indicate that this combinatorial approach also has beneficial effects in the retina in diabetes. Combinations of MTP, BRM, and DOX or TAM at doses that individually had little or no beneficial effect on the diabetes-induced increase in retinal superoxide levels resulted in a significant inhibition of the retinal oxidative stress and showed a similar, although less strong, beneficial effect on expression of proinflammatory proteins in the retina. Moreover, combinations of MTP + BRM + DOX or MTP + BRM + TAM at their DMIox mitigated a greater number of the long-term complications of DR than did individual drugs, illustrating the superiority of the combinatorial approach when drugs are applied at low dosages. We interpret that combinations of the drugs tested apparently led to stimulation of Gi/o signaling by activating the dopamine receptors D2R and D4R as well as inhibition of Gs and Gq signaling by antagonizing D1R and ADRA1A, respectively. Crosstalk is known to occur among signaling pathways, so manipulation of a particular GPCR not only affects the signaling pathways regulated by that GPCR but also can bring about changes in other signaling pathways. Manipulation of these receptors using the same drugs also had broad effects on the retinal transcriptome in retinal degeneration (Chen et al., 2016b), showing that the combined lower-dose GPCR-targeted treatments better preserved patterns of retinal gene expression that were similar to those of the normal retina than did higher-dose monotherapies.
Receptors affected by these drugs are found in the retina (Chen et al., 2013; Ruan et al., 2020), but it cannot be assumed that the beneficial effects of the drugs were mediated via drug effects in those retinal cells. The drugs used by us act also on other cell types not residing in the eye (including leukocytes), resulting in anti-inflammatory and antioxidant effects (Heijnen et al., 1996; Dunzendorfer and Wiedermann, 2000; Kintscher et al., 2001; Takahashi et al., 2005; Grisanti et al., 2011; Chen et al., 2016b; García-Prieto et al., 2017; King, 2017). Leukocytes have been implicated in the capillary degeneration and altered permeability in diabetes (Li et al., 2012; Talahalli et al., 2013; Tian et al., 2013; Veenstra et al., 2013; Liu et al., 2019a) perhaps via leukostasis, leukocyte-mediated cytotoxicity against the ECs, and release of bioactive compounds from leukocytes circulating through the retinal vasculature. The present results show that DOX monotherapy and the triple combinations of drugs statistically significantly inhibited both the leukocyte-mediated cytotoxicity against retinal ECs as well as the retinal capillary degeneration in diabetes.
The term “systems pharmacology” describes a therapeutic approach whereby multiple drugs modify different signaling pathways that act additively to achieve a positive therapeutic effect (Berger and Iyengar, 2009; Hansen et al., 2011; Chen et al., 2013, 2016a, 2016b; Orban et al., 2017). Importantly, this unbiased approach can lead to beneficial effects even when specific knowledge is lacking about the molecular mechanisms of the abnormalities in cells or tissues. Another potential advantage of the systems pharmacology approach is that combinations of certain drugs have been reported to have synergistic beneficial therapeutic effects at low drug doses (Chen et al., 2013, 2016b; Orban et al., 2018; Leinonen et al., 2019), thus minimizing potential dose-dependent side effects of the drugs.
Differences between DOX and TAM with respect to the diabetes-induced increase in permeability and between pramipexole and BRM with respect to retinal oxidative stress in the present results indicate that we cannot assume that all β- and α-adrenergic antagonists (Gs- and Gq-coupled, respectively) or D2-like dopamine-receptor agonists (Gi-coupled) individually or in combination would be effective therapeutic approaches to inhibit DR. It seems likely that BRM’s diverse receptor actions contribute to the beneficial effects of the drug on DR. BRM shows high potency also for Gi-coupled 5-HT1A and 5-HT1D receptors, and targeting these receptors with agonists has been shown to decrease oxidative stress and damage in retinal pigment epithelium and retina injury models (Collier et al., 2011; Thampi et al., 2012; Coyner et al., 2016).
A weakness of the current study is that we did not demonstrate that the lower concentrations of drugs actually reduced the risk of undesirable side effects (such as tachycardia and hypertension). Nevertheless, administration of drugs at the lowest doses that show desirable effects is an accepted tenet of pharmacology.
Early DR is not a single abnormality but is comprised of a spectrum of lesions that can occur individually in other conditions. For example, retinal vascular permeability is increased also in ischemia-reperfusion injury and age-related macular degeneration (Erickson et al., 2007; Abcouwer et al., 2013), capillary degeneration occurs also in silicosis and aging (Kuwabara et al., 1961; Soliman et al., 2015), retinal microaneurysms develop also in macroglobulinemia (Xu et al., 2015; Vasileiou et al., 2020), and dysfunction of retinal neurons develops in a variety of conditions, suggesting that these lesions do not necessarily develop by identical mechanisms and thus might not respond equally to the same therapies. The monotherapies tested had beneficial effects on some but not all components of the retinopathy, so a combination of the therapies seems best suited for having beneficial effects on the broadest spectrum of lesions. Whether higher concentrations of the individual drugs tested here might inhibit the full spectrum of lesions that characterize DR is not known, but higher drug doses are expected to increase the likelihood of side effects. We conclude that there is value in therapy development that focuses on ameliorating dysfunctions of multiple pathways and networks in DR rather than targeting single abnormalities.
Acknowledgments
The authors thank Dr. N. Sheibani (University of Wisconsin-Madison) for the immortalized mouse retinal endothelial cells (Su et al., 2003); Kathryn Zongolowicz and Heather Butler from the Case Western Reserve University National Eye Institute Core grant for the evaluation of visual function; and Aicha Saadane, Emma M. Lessieur, and Jianying Kiser for experimental and animal support.
Authorship Contributions
Participated in research design: Kern, Palczewski.
Conducted experiments: Du, Tang, Lee, Liu, Dreffs.
Performed data analysis: Kern, Du, Antonetti.
Wrote or contributed to the writing of the manuscript: Kern, Leinonen, Antonetti, Palczewski.
Footnotes
- Received March 19, 2021.
- Accepted August 3, 2021.
This work was supported by National Institutes of Health National Eye Institute [Grants EY022938, R24 EY024864, R24 EY027283, EY012021, EY011373, and EY007003]; National Institute of Diabetes and Digestive and Kidney Diseases [Grant DK020572]; and the Department of Veterans Affairs [Grant BX003604]. T.S.K. is the recipient of a Research Career Scientist award from the Department of Veterans Affairs. K.P. is the Irving H. Leopold Chair of Ophthalmology at the Gavin Herbert Eye Institute, Department of Ophthalmology, University of California, Irvine. The authors acknowledge unrestricted grants to the Department of Ophthalmology at Case Western Reserve University and at the University of California-Irvine from Research to Prevent Blindness (New York, NY).
T.S.K and K.P. are inventors of US patent no. 10272106B2 (“Compositions and methods of treating diabetic retinopathy”) issued to Case Western Reserve University. K.P. also is an inventor of related US patent nos. 8722669 (“Compounds and methods of treating ocular disorders”) and 20080275134 (“Methods for treatment of retinal degenerative disease”) issued to Case Western Reserve University. The values of these patents may be affected by this publication.
↵
 This article has supplemental material available at molpharm.aspetjournals.org.
This article has supplemental material available at molpharm.aspetjournals.org.

Abbreviations
- ADRA1A
- α1A-adrenergic receptor
- BRM
- bromocriptine
- DMIox
- dose of minimal inhibition of retinal oxidative stress
- DOX
- doxazosin
- DR
- diabetic retinopathy
- EC
- endothelial cell
- FITC
- fluorescein isothiocyanate
- GPCR
- G-protein–coupled receptor
- ICAM1
- intercellular adhesion molecule 1
- iNOS
- inducible isoform of nitric oxide synthase
- IPL
- inner plexiform layer
- MTP
- metoprolol
- OPL
- outer plexiform layer
- TAM
- tamsulosin
- Copyright © 2021 by The American Society for Pharmacology and Experimental Therapeutics





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}