Article Text

Abstract
Aims—The nuclear enzyme DNA topoisomerase II has been shown to be required for chromatin condensation and chromosomal segregation during mitosis; its isoform topo IIα is linked with active cell proliferation in mammalian cells. The aim of this study was to examine the relation of the expression of topo IIα to the biological behaviour of conventional urinary bladder cancer.
Methods—Formalin fixed, paraffin wax embedded tissue from 94 specimens of bladder urothelial cancer were immunohistochemically stained for topo IIα. For each case, a topo IIα index was determined. A similar index had been determined for Ki-67, a known cell proliferation marker. Each case had also been graded, staged, and evaluated for DNA ploidy as well as for p53 and bcl-2 immunoreactivity.
Results—Raised topo IIα expression (in ≥ 10% of malignant nuclei) correlated with two adverse prognosticators—high grade (p = 0.027) and invasion of the muscularis propria (p = 0.013), but with no other evaluated parameter. By multivariate survival analysis using Cox's proportional hazard model, high expression of topo IIα was found to be predictive for worse survival (p = 0.0047). Patients' age, tumour stage, and grade were also retained as independent prognostic factors (p = 0.0349, p = 0.00005, and p = 0.0130, respectively). The negative influence of increased topo IIα immunopositivity on patients' survival was also seen in the subgroup of patients with non-muscle invasive carcinomas (p = 0.0004), in patients with a bcl-2 negative phenotype (p = 0.0330), and in those with low Ki-67 indices (p = 0.0341).
Conclusions—Because topo IIα and Ki-67 failed to demonstrate a significant inter-relation, they appear to be different molecules that both function at separate phases in the complex process of cellular proliferation. The assessment of increased topo IIα immunoreactivity in specimens from urothelial carcinomas might help to select patients (particularly among those with superficial tumours) in the worse prognostic categories for new therapeutic strategies.
- transitional cell carcinoma
- prognosis
- DNA topoisomerase IIα
Statistics from Altmetric.com
Analysis of the cell kinetics of cancer cells in situ—for example, by mitotic counts, DNA analysis, or Ki-67 antigen expression—is used increasingly to evaluate the prognosis and/or biological behaviour of various human malignancies.1 DNA topoisomerase II (topo II) is thought to be one of these cell cycle related proteins, and topoisomerase IIα (topo IIα), one of its isoforms, has been shown to play an important role in the cell cycle through catalysing the topological isomerisation of DNA by passing one strand of DNA through a reversible break in a second DNA strand.1 Dysregulation or qualitative alterations of topo IIα expression in the cell cycle are being reported in both normal tissues and various human neoplasms.1–4 The sensitivity or resistance of a malignant cell to several antitumour drugs known as “topo II poisons” is quantitatively dependent on the cellular content of topo II.5
In addition to tumour growth fraction, another phenomenon closely linked with tumour response to chemotherapy is apoptosis because several anticancer drugs cause cell death by apoptosis and therefore require a functional apoptotic pathway. Forced overexpression of topo IIα was found to cause morphological changes in recipient cells associated with apoptosis.6 The p53 tumour suppressor gene is upregulated in cells suffering from genetic damage. Most p53 gene abnormalities (mutations) result in abrogation of the growth inhibitory or apoptotic potential of the encoded protein and thus facilitate unrestrained proliferation and progressive genomic instability.7 Because wild-type (w-t) p53 negatively regulates the minimal promoter for topo IIα,7 alterations of p53 (mutations) might result in increased transcription of topo IIα mRNA and a concomitant increase in protein concentrations, which could confer a growth advantage. The simultaneous comparative assessment of DNA content is of interest because aneuploidy might be associated with aberrations involving chromosome 17,7 which contains the loci encoding p53 and topo IIα. The immunohistochemically detectable bcl-2 oncoprotein is encoded by a gene involved in the t(14;18) chromosomal translocation; it plays a central role in apoptosis, acting as an inhibitor of several apoptotic processes.8
Classic clinicopathological features of urinary bladder cancer, such as staging and grading, are crucial in stratifying patients for treatment. Therapeutic advances indicate a need for more accurate prediction of tumour behaviour, especially of superficial bladder cancers in individual patients; therefore, new, additional prognostic indicators are worth investigating. In this study, we performed immunohistochemical analysis of topo IIα in 94 patients with transitional cell carcinomas (TCCs) of the urinary bladder in whom the postoperative course had been documented, and compared those findings with various clinicopathological parameters, including p53 and bcl-2 immunostatus, and with specific survival of the patients. Because topo IIα concentrations are thought to be highest in proliferating cells, and the Ki-67 antigen (an accepted marker of proliferation) and DNA content of neoplastic cells have been shown to have some prognostic importance in urothelial cancer,9 we also took into account the Ki-67 immunoexpression and DNA ploidy in the examined specimens.
Methods
PATIENTS AND TUMOURS
Our study included 94 patients with TCC of the bladder. Paraffin wax embedded, formalin fixed blocks from biopsies or surgically resected specimens were retrieved and haematoxylin and eosin stained sections were reviewed to ensure the accuracy of the diagnosis. Selection was based on the availability of sufficient material for immunohistochemistry. The grade was assigned according to the World Health Organisation system,10 and represented the highest grade present in the examined material. Pathological staging was performed based on the AJCC/UICC criteria.9 Carcinoma in situ occurred only in association with TCCs of other stages in the selected cases. Tumours were also divided into two groups: “superficial” (stages Ta and T1) and “muscle invasive” TCCs (stages T2, T3a, and T3b) because the most important task of local staging is to determine whether the muscularis propria has been invaded; this is the single most crucial piece of information for therapeutic decision making. Patients with non-invasive papillary TCCs (stage Ta) were treated by transurethral resection and fulguration of the visible tumours, and stage T1 patients were treated by transurethral resection with adjuvant intravesical treatment. Muscle invasive TCCs were treated by radiotherapy or total cystectomy. All patients were examined at least three times a year; the median follow up time was 36 months (10–88), the last update including all details being 1 October 1999. Survival was expressed as the number of months from the date of first cystoscopy to the occurrence of death as a result of (or with) advanced bladder cancer (specific survival).
IMMUNOHISTOCHEMICAL STAINING
Immunohistochemistry for topo IIα was performed using a monoclonal anti-topo IIα antibody (topo IIα, clone JH2.7, diluted 1/100; Biocare Medical, San Diabolo, California, USA). Sections of 5 μm thickness were studied. Dewaxed sections were heated in 0.01 M citric acid (pH 6.0) for two times five minutes in a microwave oven at maximum power. Slides were washed at room temperature and incubated overnight at 4°C with the primary antibody. A standard avidin–biotin–peroxidase complex (ABC) technique (Vectastain Elite; Vector Laboratories, Burlingame, California, USA) was used for visualisation with diaminobenzidine as a chromogen. Sections were counterstained with haematoxylin and mounted. Tonsil samples from our routine files were used as positive controls for topo IIα. First, immunolabelling was evaluated light microscopically using a ×20 objective, by an experienced pathologist unaware of the clinical data. The topo IIα index for each TCC was assessed by counting the proportion of topo IIα positive cells from 400 to 1000 (average 650) neoplastic cells from a morphologically well presented area. In addition, each topo IIα index was verified and occasionally modified by image analysis on each slide. Images were acquired using an Olympus BX40 microscope with a mechanical stage, fitted with a SONY-iris CCD videocamera controlled by a Dipix P360F framegrabber/display card in a pentium II personal computer. The measurements were performed with the Image Scan Software (Jandel Scientific, Erkrath, Germany). For topo IIα scores, the cut off point was selected at 10%, according to the median value rounded off to the nearest 5%.
The p53 and bcl-2 immunoexpression status of the TCCs included in our study were available from a previous study,11 in which we had chosen to interpret any TCC with ≥ 10% of the tumour cells showing nuclear p53 staining to be positive for an underlying missense mutation in the gene. A p53 index of < 10% had identified a TCC with a normal p53 gene. The method of flow cytometry, according to the Becton Dickinson protocol, had also been previously undertaken and the TCCs had been defined as either aneuploid or near diploid according to their DNA content.12
STATISTICS
Data were entered on to a computerised database and analysed by the SPSS statistical package. Pearson's χ2 test with continuity correction was used to evaluate the topo IIα expression as a categorical variable with regard to the variables of interest. Survival rates were assessed by the log rank test (univariate statistics) as well as by Cox's proportional hazard regression model (multivariate statistics).
Results
In general, topo IIα staining was seen as a totally distinct, diffuse nuclear pattern (fig 1). Topo IIα indices ranged from a low of < 1% to a high of 35% (mean, 7.73%; SD, 8.16%). When tumour adjacent urothelium could be studied, the topo IIα expression was almost negative. High topo IIα expression (topo IIα indices ≥ 10%) was more frequently detected in muscle invasive TCCs and this difference was significant (p = 0.013; table 1). With regard to the three tumour grades, the incidence of TCCs with high topo IIα immunoreactivity increased as tumour differentiation became poorer (p = 0.027; table 2). No difference was noticed between topo IIα immunostaining status (< 10% or ≥ 10%) and other assessed variables (patient's sex (p = 0.117), p53 immunostatus (p = 0.16), bcl-2 immunostatus (p = 0.8), Ki-67 index (p = 0.7), or DNA ploidy (p = 0.7)).
Differences of topoisomerase IIα expression between the groups of superficial and truly invasive tumours
Differences in topoisomerase IIα immunopositivity three groups of patients with different tumour grades

Distinct nuclear positivity for topoisomerase IIα in cancerous cells of a low grade transitional cell carcinoma (avidin–biotin–peroxidase complex; magnification, ×400).
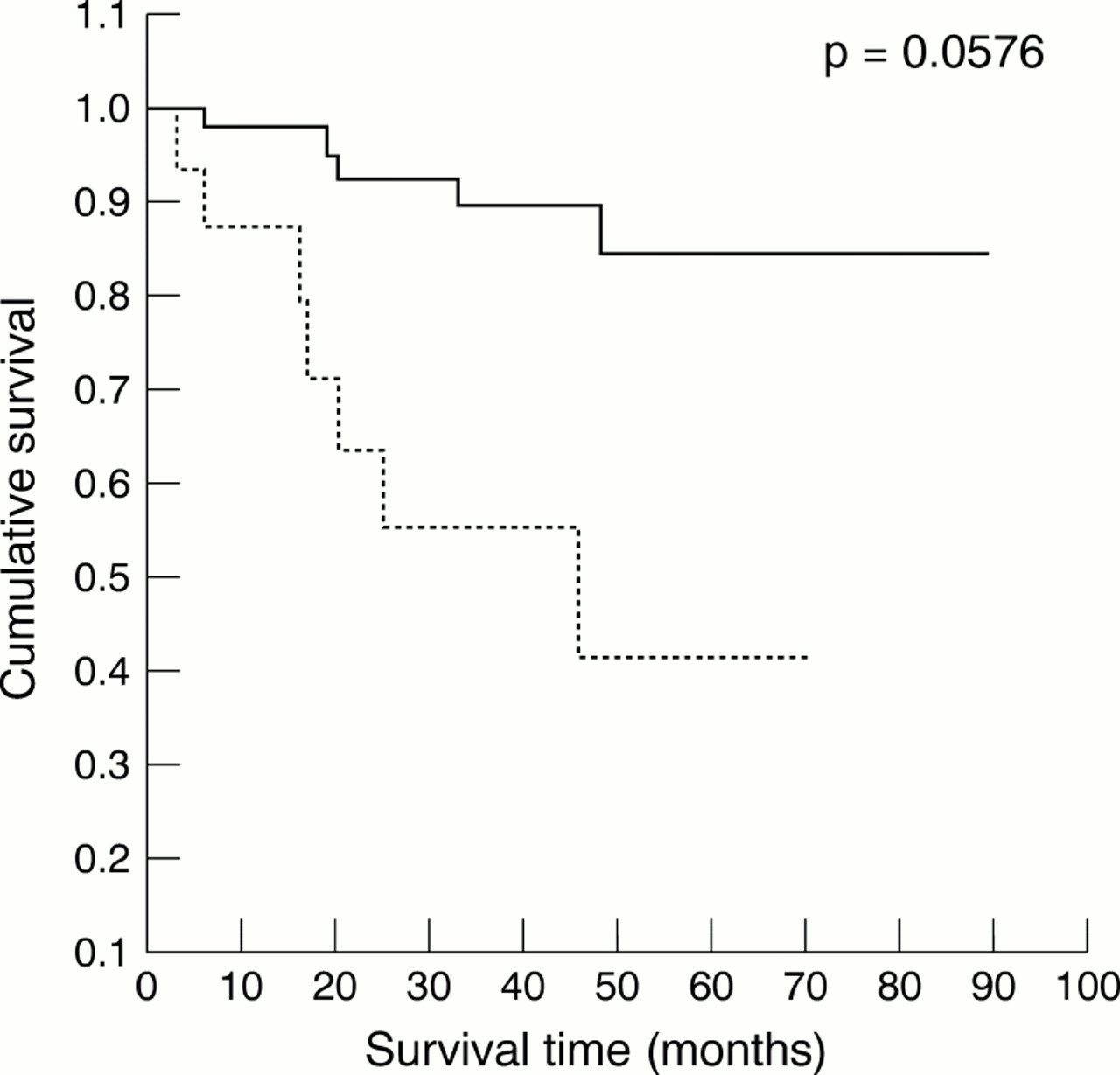
Topo IIα was the only immunomarker (of the four evaluated in our study) that was related to patients' specific survival. In detail, patients' survival was found to be significantly influenced by patients' age (p = 0.0349), tumour stage and grade (p = 0.00005 and p = 0.0130, respectively) and, interestingly, by topo IIα immunostatus (p = 0.0047) (multivariate analysis, Cox's model; table 3). In other words, the risk of death was generally increased in the group of patients with high topo IIα expression in their tumours (fig 2). Moreover, in specific patient subgroups the following observations were made: (1) Among patients with low Ki-67 scores, those with synchronous low topo IIα expression in their TCCs survived significantly longer (p = 0.0341; fig 3A). (2) Among patients with superficial tumours, the ones with tumours expressing topo IIα in < 10% of neoplastic cells survived even longer (p = 0.0004; fig 3B). Patients with loss of bcl-2 expression in their TCCs survived relatively longer when topo IIα expression was low (p = 0.0330; fig 3C).
Cox's regression analysis for independent prognostic variables with respect to patients' specific survival (dependent variable)

Survival of patients with topoisomerase IIα indices ≥ 10% (dotted line) and < 10% (solid line) in human bladder carcinomas.

{kind=link}
{kind=link}
{kind=link}
The influence of topoisomerase IIα (topo IIα) expression on the survival of specific patient subgroups. (A) Transitional cell carcinomas (TCCs) with low Ki-67 indices; (B) superficial TCCs; (C) Bcl-2 negative TCCs. Dotted line, topo IIα expression ≥ 10%; solid line, topo IIα expression < 10%.
Discussion
DNA topo II is an essential cellular enzyme that functions in the segregation of newly replicated chromosome pairs, in chromosome condensation, and in altering DNA superhelicity.13 Because the expression of the topo IIα isoform increases during the late S phase, decreases at the end of the M phase, and is dramatically reduced in the G1/G0 phase of the cell cycle,14 an anti-topo IIα antibody labels cells in the S, G2, and M phases of the cell cycle.13 The immunohistochemical method for the in situ determination of topo IIα has been validated extensively and shown to reflect closely the exact enzyme activity in formalin fixed paraffin wax embedded human tissues.15 On the contrary, techniques such as western or northern blotting are averaging techniques and do not assess the amount of topo II in one particular neoplastic cell.
In general, the biological behaviour of human malignancies is influenced by two major biological features of cancer cells: abnormal proliferation and the potential to invade and metastasise, which occasionally correlate with each other. In our study, we examined a cell proliferation immunomarker, topo IIα, with regard to the invasion of bladder muscularis propria by the tumour cells. High topo IIα expression was more frequently detected among muscle invasive TCCs (p = 0.013), which behave more aggressively than muscle non-invasive tumours. To the best of our knowledge, such a correlation has not been studied previously. However, this difference in the prevalence of high topo IIα immunoreactivity did not remain significant when the specific AJCC/UICC stages were analysed separately.
With regard to the degree of tumour differentiation, the incidence of high topo IIα immunopositivity was significantly greater in high grade TCCs (p = 0.027). This strong correlation is in agreement with one previous study in urothelial cancer,3 as well as in other malignancies.5, 15 In malignant cells, overexpression of the topo IIα protein might reflect not only the proliferative advantage of these cells, but also qualitative alterations caused by malignant transformation and dedifferentiation.13 In a recent study, treatment of the hepatoma cell line Hep3B with retinoids (which can induce cell differentiation) appeared to have a direct effect on the topo IIα gene promoter because it greatly reduced both the steady state amount of mRNA and the transcription rate of the topo IIα gene.16
Apart from tumour stage and grade, the proliferative activity of malignant cells might also correlate with prognosis in urotherlial cancer.9 As regards the two evaluated proliferation markers (topo IIα and Ki-67), they were not significantly related to each other and their scores were not closely covariant. Ki-67 indices simply followed the same distribution pattern as topo IIα in that the highest indices were in the high grade group and the lowest indices were in the low grade group. Nevertheless, Ki-67 indices were always higher than the respective topo IIα indices. Therefore, although the overall staining pattern between topo IIα and Ki-67 is similar within each histological grade, the striking quantitative divergence suggests that these two molecules are separate entities. In fact, sequence data have shown that the genetic sequence of Ki-67 has no homology to that of topo II.3 The lower topo IIα labelling indices might be the result of assay sensitivity. Topo IIα structure and its mechanism of activity are well understood.17 In detail, because the expression of topo IIα dramatically increases in the late S phase and decreases rapidly at the end of the M phase,2 this results in less variation, especially in archival tumour specimens. On the contrary, Ki-67 antigen is present in all phases of the cell cycle (late G1, S, M, and G2 phases) except G0. Therefore, topo IIα, being present only during the late S and G2 phases of the cell cycle, might give a better estimate than Ki-67 of the number of actively cycling cells.
Deregulation of topo IIα expression is known to result in apoptotic cell death.6 As far as the apoptosis related proteins are concerned, no topo IIα correlation, positive or negative, emerged with either p53 or bcl-2 immunostatus. In cell line studies, the steady state level of topo IIα mRNA decreased after the expression of w-t p53, but not mutant p53, suggesting that the repression of topo IIα mRNA synthesis could be one mechanism by which mammalian cells regulate progress through the cell cycle, particularly after exposure to cytotoxic stresses that upregulate p53 activity.16 However, in our cases no association between high topo IIα immunoexpression and p53 positive immunostatus was detected. To the best of our knowledge, there is no other immunohistochemical study that compares p53 and topo IIα; thus, our negative findings are not comparable with those of the study above. Moreover, topo IIα immunoexpression was not linked with bcl-2 immunostaining. This negative finding is supported by another study in which apoptosis mediated by topo IIα deregulation could not be blocked by bcl-2.6 This lack of inhibition of topo IIα mediated cell death by bcl-2 indicates that the onset of cell death is mediated by distinct apoptotic signal transduction pathways.
The Cox's proportional hazard regression model revealed that patients' age, tumour stage, and grade as well as topo IIα immunoreactivity had a significant influence on mortality. Using a cut off point of 10%, the topo IIα immunostatus significantly differentiated outcomes (p = 0.0047). Consequently, we can presume that TCCs with high topo IIα expression were characterised by increased biological aggressiveness. Interestingly, for Ta and T1 TCCs, which are usually treated conservatively, high topo IIα expression has been found to be a powerful indicator of adverse prognosis.
It is noteworthy that high topo IIα expression retained its negative influence on the survival of specific patient subgroups. One of the latter consisted of patients whose neoplastic cells had a bcl-2 negative immunophenotype. Loss of bcl-2 expression in TCCs is a potentially ominous prognosticator, although not independent with respect to survival11; however, in other malignancies, such as small cell lung cancer,17 lower survival probability has been observed in patients with bcl-2 positive cancers. Among patients with rather low Ki-67 immunopositivity, an increase in topo IIα expression was found to be predictive of worse survival.
In conclusion, high topo IIα immunoexpression was associated with biologically aggressive TCCs and appears to be an independent, significant, unfavourable predictor with respect to specific survival in patients with bladder cancer, especially those with superficial TCCs. Therefore, in the future, such patients might benefit from more aggressive treatment and may need more intense follow up.