Article Text

Abstract
Evidence is presented to support the proposal that activation of the type 1 vanilloid receptor (VR1) is an important sensory mechanism in cough.
- cough
- vanilloid receptor (VR)-1
Statistics from Altmetric.com
Cough is the commonest respiratory symptom. According to the 1992 morbidity statistics in general practice, acute “viral” cough accounts for the largest single cause of new consultations with GPs with an annual expenditure in 1999 of more than £200 million in the UK, mostly on medicines which are, at best, poorly effective. Chronic cough arises from a number of different pathologies and is a common and problematic source of referral to chest physicians. However, despite half a century of research, the pathophysiological mechanisms causing cough are poorly understood. In particular, the receptor that stimulates the afferent arm of the cough reflex has not been characterised in detail.
CAPSAICIN-LIKE DRUGS CAUSING COUGH
In man, inhalational cough challenge has been used since 19541 to study the profile of agonists and inhibitors of the reflex. These peripherally acting stimulants—which presumably act on or in close association with the putative sensory receptor—can be divided into two broad groups: (1) organic and inorganic acids and (2) agonists of the type 1 vanilloid receptor (VR1) such as capsaicin and resinoferatoxin. These latter agents are the most potent stimulants of the cough reflex so far described in man.2,3 Type 1 vanilloid receptors have been intensively studied in their role as the mediators of pain in skin and other tissues.4,5 When these receptors are exposed to noxious stimuli they act as ion channels with increased permeability to Na+ and Ca2+ ions. This influx of ions causes neuronal depolarisation and caudal propagation of action potentials. It is our belief that VR1 activation is the primary sensory mechanism in cough, and recent evidence has suggested how factors known to promote cough may act through this common pathway.
We have previously studied the mechanism of acid induced cough in man. In subjects undergoing cough challenge there is a significant correlation between different acids associated with their ability to donate protons. In contrast, there is no correlation with capsaicin responses.6 This finding could be taken as evidence for two separate mechanisms, but the capsaicin antagonist capsazepine has been found to inhibit both citric acid and capsaicin induced cough in animals.7 Thus, both capsaicin and protons appear to be acting through a common pathway, albeit at different allosteric sites. Recent advances in the understanding of the molecular activity of VR1 have indicated how these observations can be unified to produce a coherent description of a putative cough receptor.
THE TYPE 1 VANILLOID RECEPTOR (VR1)
VR1 has been cloned4 and is structurally related to the transient receptor potential family of ion channels. Rat VR1 consists of 432 amino acids and is predicted to have six transmembrane spanning domains. When expressed in cell lines not containing constitutive vanilloid receptors, patch clamping studies have confirmed that it acts as a non-specific ion channel with similar electrophysiological properties to the native receptor.4,8 In particular, the opening probability of VR1 increases not only with exogenous capsaicin but also in response to noxious stimuli such as protons and heat. The site of proton binding was identified by site directed mutagenesis on the extracellular aspect of the fifth transmembrane domain near the putative pore forming region.9
VR1 has been shown to be sensitive to a fall in the extracellular pH, and H+ ions not only stimulate the receptor directly8 but also increase the sensitivity of the receptor to capsaicin.4 Since cough may be stimulated by the direct application of acid to the airway, this implies that, if VR1 is important in cough, an endogenous capsaicin-like ligand must also be present. A number of putative ligands have been suggested, usually lipids because of the hydrophobic nature of capsaicin. Anandamide, the endogenous agonist of the cannabinoid receptor, does appear to have some activity on VR1 in vitro but, when inhaled by a single capsaicin sensitive subject, did not have any demonstrable activity apart from an unpleasant taste. That anandamide is unlikely to be the endogenous full agonist of VR1 has been confirmed in other systems and, indeed, may even inhibit cough.10
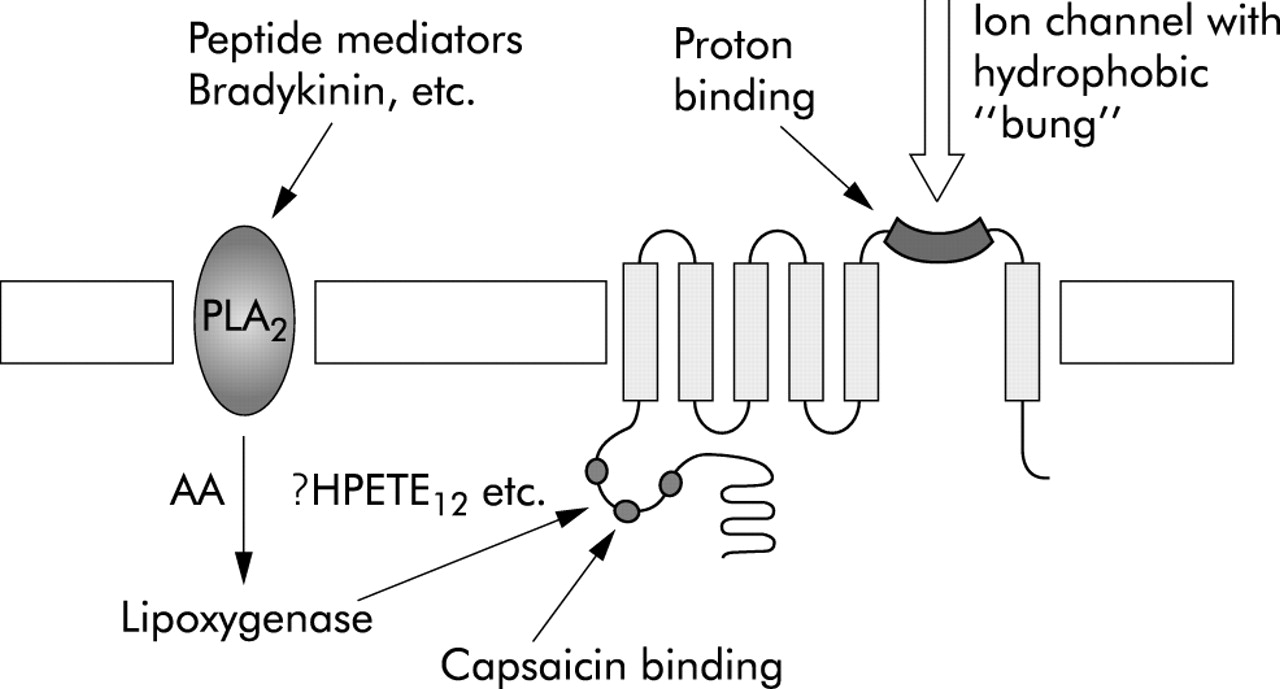
An important advance in our understanding of the biology of VR1 was the demonstration that the capsaicin binding site was located on the cytosolic domain of the receptor.11 Thus capsaicin, unlike most other ligands, traverses the cell membrane and stimulates VR1 intracellularly (fig 1). It was logical therefore for the search for the endogenous capsaicin-like ligand to be directed within the neurone. It has now been shown that lipoxygenase products are potent agonists at the capsaicin binding site.12
{kind=link}
The putative type 1 vanilloid cough receptor (VR1) illustrating possible regulation by inflammatory mediators capsaicin and protons. AA = arachidonic acid; HPETE = hydroperoxyeicosatetraenoic acid; PLA2 = phospholipase A2.
ENDOGENOUS LIGANDS OF VR1
The lipoxygenase enzymes catalyse the conjugation of a hydroperoxide moiety with arachidonic acid to produce one of a family of hydroperoxyeicosatetraenoic acids (HPETE). In asthma, 5-lipoxygenase produces 5-HPETE which is the precursor of the leukotrienes. However, there are a number of other lipoxygenase products named after the position of conjugation with arachidonic acid. In animal species from molluscs to mammals, HPETEs have been shown to regulate neurotransmission by increasing the opening probability of ion channels such as K+ channels.13–15 Patch clamping studies have shown that 12-HPETE is endowed with many of the characteristics that would be predicted for an endogenous capsaicin-like ligand. 12-HPETE strongly activates single channel currents with an identical current voltage relationship to capsaicin. As with capsaicin, Na+ and K+ ions are conducted and capsazepine blocks the opening of the channel. These studies were performed in primary culture of dorsal root ganglia of the rat and, while 12-HPETE was the most potent putative ligand, other lipoxygenase products including LTB4 were also active. More recently we have shown that another lipid derivative, N-arachidonoyl-dopamine (NADA), activates VR1 in different animal models and also at the recombinant human VR1 more potently than anandamide and lipoxygenase derived molecules.16 However, it is not known whether NADA is the most potent endogenous ligand of human VR1.
Inflammatory stimuli—including prostaglandins, bradykinin, nerve growth factor, and others—have been shown to upregulate the expression and function of VR1 via the activation of p38MAPK, PLC-γ, PKC-ϵ, and PKA dependent pathways.17–19 Chronic airway inflammation such as that present in asthma, COPD, and other lung diseases may therefore exaggerate the sensitivity of VR1 to its agonists which, in these conditions, may reach a concentration sufficient to trigger the VR1 dependent cough reflex.
CONCLUSIONS
There is a convincing case for the promotion of VR1 as the lead candidate to be the first cloned and characterised cough receptor. The final proof must await the development of a potent and specific antagonist for use in man. It is unlikely that VR1 activation is the only stimulus for cough since some tussogenic agents such as distilled water are not inhibited by VR1 antagonism.7 That VR1 is a member of a growing family of structurally similar ion channels suggests a heterogeneous system which will require further dissection if we are to understand the biochemical basis of cough in health and disease.